Have you ever felt tingling, numbness, or weakness in your hand and wondered whether it’s just fatigue—or something more serious? Many people assume nerve-related symptoms in the arm or hand automatically mean carpal tunnel syndrome. However, another condition called Thoracic Outlet Syndrome can cause very similar symptoms, making diagnosis confusing and sometimes delayed.
Both conditions affect nerves and can significantly impact your daily life. They can make simple activities like typing, driving, or even holding a phone uncomfortable or painful. Without proper diagnosis and treatment, these symptoms may worsen over time and reduce mobility, strength, and overall quality of life.
Understanding the differences between these conditions is essential for getting the right treatment. Although they share overlapping symptoms, they originate in completely different parts of the body and require different treatment approaches. An incorrect diagnosis may result in ineffective treatment and extended discomfort.
In this comprehensive guide, you will learn the key differences between these two conditions, including symptoms, causes, risk factors, diagnostic methods, and treatment options. By the end, you will have the knowledge needed to recognize warning signs early and seek the appropriate care for faster relief and long-term recovery.
Understanding Carpal Tunnel Syndrome
Carpal tunnel syndrome is one of the most common nerve compression disorders, affecting millions of people worldwide. It happens when the median nerve is compressed while traveling through the carpal tunnel in the wrist.
This tunnel is a narrow passage made of bones and ligaments. When inflammation, swelling, or structural changes occur, pressure builds up and compresses the nerve.
Anatomy and Mechanism
The median nerve controls sensation and movement in several parts of the hand. When compressed, it affects:
- Thumb
- Index finger
- Middle finger
- Part of the ring finger
This compression disrupts nerve signalling, leading to sensory and motor symptoms.
Key anatomical features involved:
- Median nerve
- Carpal tunnel ligament
- Wrist bones
- Tendons surrounding the nerve
According to the Mayo Clinic, prolonged pressure on the median nerve leads to progressive symptoms if left untreated.
Common Symptoms of Carpal Tunnel Syndrome
Symptoms often develop gradually and worsen over time. Many patients first notice symptoms at night or during repetitive activities.
Most common symptoms include:
- Tingling or numbness in fingers
- Hand weakness
- Difficulty gripping objects
- Pain radiating up the arm
- Frequent dropping of objects
Symptom pattern clues:
- Symptoms worsen at night
- Shaking the hand provides temporary relief
- Symptoms affect thumb, index, and middle fingers
If untreated, muscle weakness and permanent nerve damage may occur.
Causes and Risk Factors
Carpal tunnel syndrome develops due to increased pressure within the wrist tunnel.
Common causes include:
- Repetitive hand movements
- Typing or computer work
- Wrist injuries
- Arthritis
- Diabetes
- Pregnancy-related swelling
High-risk professions:
- Office workers
- Assembly line workers
- Drivers
- Musicians
- Healthcare professionals
Early intervention can prevent progression and permanent nerve damage.
What Is Thoracic Outlet Syndrome?
This condition affects the nerves or blood vessels located between the collarbone and the first rib. This area is known as the thoracic outlet, and compression here can disrupt nerve and vascular function.
Unlike carpal tunnel syndrome, which affects the wrist, this condition originates near the neck and shoulder region.
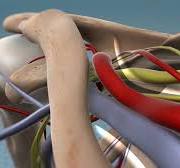
Anatomy of the Thoracic Outlet
The thoracic outlet contains critical structures including:
- Brachial plexus nerves
- Subclavian artery
- Subclavian vein
- Muscles and bones
Compression in this area affects nerve signals traveling from the neck to the arm.
Types include:
- Neurogenic (most common)
- Venous
- Arterial
According to the Cleveland Clinic, neurogenic type accounts for over 90% of cases.
Symptoms Originating from the Neck and Shoulder
Symptoms often begin in the shoulder and travel downward into the arm.
Common symptoms include:
- Neck pain
- Shoulder tightness
- Arm fatigue
- Tingling in fingers
- Weak grip strength
Unique distinguishing signs:
- Symptoms worsen when raising arms
- Shoulder discomfort precedes hand symptoms
- Pain may involve entire arm
These symptoms can mimic other nerve disorders, which makes diagnosis challenging.
Causes and Risk Factors
This condition can develop due to structural abnormalities or repetitive strain.
Common causes include:
- Poor posture
- Neck injuries
- Repetitive overhead activities
- Trauma
- Anatomical abnormalities
High-risk individuals include:
- Athletes
- Office workers with poor posture
- People with neck injuries
- Weightlifters
Early diagnosis improves recovery outcomes.
Key Differences Between the Two Conditions
Recognizing the differences is crucial for ensuring proper treatment and effective recovery.
Location of Nerve Compression
Carpal tunnel syndrome:
- Compression occurs in wrist
- Affects median nerve only
Thoracic outlet-related compression:
- Occurs near neck and shoulder
- Affects brachial plexus nerves
This difference explains the variation in symptom patterns.
Symptom Distribution
Carpal tunnel syndrome symptoms typically affect specific fingers.
Thoracic outlet-related symptoms may affect the entire arm.
Comparison:
| Feature | Carpal Tunnel | Thoracic Outlet Related |
| Origin | Wrist | Neck/Shoulder |
| Fingers affected | Specific | Entire arm possible |
| Neck pain | Rare | Common |
| Shoulder pain | Rare | Common |
Activity Triggers
Carpal tunnel syndrome worsens with wrist activity.
Thoracic outlet-related compression worsens with arm elevation.
Examples:
- Typing worsens wrist-related compression
- Overhead lifting worsens outlet compression
Understanding triggers helps differentiate between the two.
Diagnosis and Testing Methods
Accurate diagnosis is essential for effective treatment.
Physical Examination
Doctors evaluate:
- Muscle strength
- Sensory response
- Reflexes
- Range of motion
These tests help identify nerve involvement.
Imaging and Nerve Testing
Common diagnostic tools include:
- MRI
- X-ray
- Nerve conduction studies
- Ultrasound
These tests locate compression areas.
Differential Diagnosis
Doctors must rule out:
- Cervical spine disorders
- Peripheral neuropathy
- Other nerve compressions
Accurate diagnosis ensures proper treatment.
Treatment Options and Recovery
Treatment depends on severity and cause.
Conservative Treatment
Most patients improve without surgery.
Non-surgical treatments include:
- Physical therapy
- Posture correction
- Anti-inflammatory medications
- Activity modification
These treatments reduce nerve compression.
Physical Therapy and Rehabilitation
Therapy focuses on improving alignment and reducing pressure.
Goals include:
- Strengthening muscles
- Improving posture
- Reducing inflammation
- Restoring nerve function
Consistent therapy improves outcomes.
Surgical Treatment Options
Surgery is recommended if conservative treatment fails.
Procedures may include:
- Nerve decompression
- Removal of compressive structures
Surgery success rates are high when properly indicated.
Prevention Strategies for Long-Term Relief
Preventing nerve compression requires lifestyle adjustments.
Posture Improvement
Good posture reduces nerve pressure.
Tips include:
- Keep shoulders relaxed
- Avoid slouching
- Maintain neutral wrist position
Proper posture prevents recurrence.
Ergonomic Adjustments
Workplace ergonomics plays a crucial role.
Important adjustments include:
- Proper chair height
- Wrist support
- Monitor positioning
Ergonomics reduces nerve stress.
Exercise and Strengthening
Regular exercise improves muscle balance.
Helpful exercises include:
- Stretching
- Strengthening routines
- Mobility exercises
Exercise promotes nerve health.
When to See a Specialist for Thoracic Outlet Syndrome
Early medical evaluation prevents long-term complications. Many patients ignore symptoms until weakness or chronic pain develops, which makes treatment more complex and recovery slower.
You should consult a specialist if symptoms persist beyond a few weeks or worsen over time. Early diagnosis helps reduce the risk of permanent nerve damage and enhances treatment outcomes.
Seek medical care if you experience:
- Persistent numbness or tingling
- Arm weakness
- Shoulder pain
- Reduced grip strength
- Symptoms interfering with daily activities
A specialist can perform diagnostic tests and recommend the most effective treatment plan based on your condition.
Conclusion
Nerve compression disorders can significantly affect daily function, comfort, and quality of life. Understanding the differences between carpal tunnel syndrome and Thoracic Outlet Syndrome is essential for accurate diagnosis and effective treatment. While both conditions share similar symptoms, their causes, locations, and treatment approaches differ.
Early diagnosis and proper treatment can prevent long-term complications and restore normal function. If you experience persistent symptoms such as numbness, weakness, or pain, seeking medical evaluation is the best step toward recovery. Book your consultation today and take the first step toward lasting relief and improved nerve health.